Melanoma
Melanoma is cancer that usually occurs on the skin. It develops from the cells that produce the dark-colored pigment melanin, which is responsible for our skin's coloring. Ocular melanoma is often lethal, but thankfully very rare disease. Many people die from it, especially when it spreads to the liver, a common complication. There are other types of eye cancers, but melanoma is the most common. Choroidal melanomas are the most common site comprising 85% of cases. Other sites include ciliary body, iris, and conjunctiva.
Ocular Melanoma Overview
Melanoma is cancer that usually occurs on the skin. It develops from the cells that produce the dark-colored pigment melanin, which is responsible for our skin's coloring.
These cells, called melanocytes, are also found in other places in our bodies, such as our hair, the lining of our internal organs, and our eyes. So while most melanomas do begin to grow in the skin, it is possible for a melanoma to begin in other parts, including the eye. When melanoma does occur in the eye it is called ocular melanoma.
Ocular melanoma is often lethal, but thankfully very rare disease. Many people die from it, especially when it spreads to the liver, a common complication. There are other types of eye cancers, but melanoma is the most common. Choroidal melanomas are the most common site comprising 85% of cases. Other sites include ciliary body, iris, and conjunctiva.
Current research is also showing that ocular melanoma is very different from normal skin melanoma.
Who is at risk for ocular melanoma?
Around 2,500 people are diagnosed every year in the United States. In both the U.S. and Europe, this equates to about 5 - 7.5 per million people per year; for people over 50 years old the incidence rate is increased to around 21 per million per year.
What is an eye tumor?
A tumor is simply a mass or tissue swelling. The term applies to benign (noncancerous) tumors, such as a mole on the skin, as well as malignant tumors, also called cancers, that occur when cells grow abnormally and possibly spread to other parts of the body.
A benign tumor does not have the ability to invade or spread to other organs. Benign tumors are not cancers.
A malignant tumor, however, does have the ability to invade and spread to other organs. A malignant tumor is cancer.
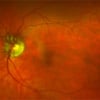
Choroidal melanoma is the most common primary intraocular (occurring inside the eye) tumor in adults. It arises from the pigmented cells of the choroid of the eye and is not a tumor that started somewhere else and spread to the eye.
A choroidal melanoma is malignant. It is cancer that may metastasize and spread to other parts of the body. Because choroidal melanoma is intraocular and not usually visible, patients with this disease often do not recognize its presence until the tumor grows to a size that impairs vision by obstruction, retinal detachment, hemorrhage, or other complication. Pain is unusual, except with large tumors.
Periodic retinal examination is the best means of early detection. Few people realize that your eye doctor can save your life by detecting this problem in its early stages.
How is ocular melanoma treated?
The treatment for intraocular melanoma depends on the size and location of the tumor, whether the cancer has spread, and the person's overall health. The main reasons for treating intraocular melanoma are to reduce the risk of the tumor spreading and maintain the health and vision of the eye, if possible. In many cases, a team of doctors may work with the patient to determine the best treatment plan.
Observation
This approach may be used to manage small or slow-growing tumors, or for people without any symptoms, older or seriously ill people, or people with a tumor in their only useful eye. If the tumor grows bigger than 10 mm in diameter or 2 mm to 3 mm in height (thickness), then the doctor and the patient may decide to proceed with treatment.
Surgery
Surgery to the eye is quite common in the treatment of intraocular melanoma. During surgery, the ophthalmologist will remove parts of the affected eye or even the entire eye, depending on the size and spread of the tumor.
-
Iridectomy: Removal of part of the iris
-
Iridocyclectomy: Removal of part of the iris and ciliary body
-
Sclerouvectomy/endoresection: Surgery to remove the choroidal tumor and still keep the eye
-
Enucleation: Removal of the eye
Surgery is also used to place the radioactive plaque for internal radiation therapy (brachytherapy). (More information about radiation therapy is below.)
The potential side effects of eye surgery are similar to that of any surgery, including a risk of infection, problems from the anesthesia (the medication that puts you "to sleep" during surgery), and pain. With total removal of the eye, there is a slight risk that the tumor could come back around the edges of the eye area.
Having an eye removed (enucleation)
Sometimes the only choice a doctor has in treating intraocular melanoma is to remove the eye. This means that the person will lose all of their vision in that eye. Because of this vision loss, a person with one eye may have trouble with depth perception and may not be able to see as well when looking straight ahead. Most people adjust to these differences within a year after having the surgery.
Many people worry about what they will look like when they have an eye removed. The cosmetic surgery available today usually yields good cosmetic results. To fill the area left by the missing eye, the person is fitted for an artificial plastic eye (prosthesis). The prosthesis will look and behave almost the same as a natural eye. For example, the plastic eye will move along with the person's remaining eye, just not as much as a natural eye moves. Family members may be able to tell that the eye is not real, but it is unlikely that strangers will know. It may take many weeks for patients to receive the prosthesis.
Radiation therapy/radiotherapy
Radiation therapy uses radiation to kill or damage cancer cells. There are different types of radiotherapy.
-
Proton beam or charged particle radiotherapy targets high-energy particles to the tumor. Unlike x-rays, this type of radiation can be directed at the tumor, which reduces the possibility of damage to nearby tissue.
-
Brachytherapy is a procedure where the ophthalmologist places a radioactive disc (sometimes called a plaque) near the tumor. Sometimes this is called internal radiation therapy or plaque therapy.
-
Traditional external beam radiation therapy delivers x-rays from outside the body to the tumor and may be given after enucleation or as a palliative treatment.
Radiation therapy can result in a variety of side effects, so it is important to talk to your ophthalmologist about what to expect. The extent of side effects depends on the type and dose of radiation the patient receives, where the tumor is located, and the patient's general health. The side effects may not show up right away.
-
Cataracts are very common. A cataract is when the lens of the eye becomes cloudy. People with cataracts may have cloudy or foggy vision, have trouble seeing at night, or have problems with glare from the sun or bright lights. If the cataract is causing major problems with a person's eyesight, it can be surgically removed.
-
Loss of eyelashes and/or a dry eye can occur with external beam radiation.
These side effects are much less common and can cause a loss of vision.
-
Radiation retinopathy: The development of abnormal blood vessels in the retina
-
Radiation optic neuropathy: Optic nerve damage
-
Neovascular glaucoma: A painful condition where new blood vessels develop and block the regular release of fluid from the eye
If there is significant damage to the eye from radiation, the eye may need to be removed.
Laser therapy
This procedure uses heat in the form of a laser to shrink smaller tumors. It may also be called thermotherapy or transpupillary thermotherapy (TTT). This treatment potentially has fewer side effects than surgery or radiation.
Clinical trials
Doctors are always looking for better ways to treat patients with eye cancer. A clinical trial is a way to test a new treatment in order to prove that it is safe, effective, and possibly better than a standard treatment. Patients who participate in clinical trials are among the first to receive new treatments before they are widely available. However, there is no guarantee that the new treatment will be safe, effective, or better than a standard treatment.
Patients decide to participate in clinical trials for many reasons. For some patients, a clinical trial is the best treatment option available. Because standard treatments are not perfect, patients are often willing to face the added uncertainty of a clinical trial in the hope of a better result. Other patients volunteer for clinical trials because they know that this is the only way to make progress in treating eye cancer, such as finding new therapies. Even if they do not benefit directly from the clinical trial, their participation may benefit future eye cancer patients.
In order to join a clinical trial, patients must complete a learning process known as informed consent. During informed consent, the doctor should list all of the patient's options, so that the person understands the standard treatments, and how the new treatment differs from the standard treatment. The doctor must also list all of the risks of the new treatment, which may or may not be different than the risks of standard treatment. Finally, the doctor must explain what will be required of each patient in order to participate in the clinical trial, including the number of doctor visits, tests, and the schedule of treatment.